(Quotations in this post are from the excellent article at the bottom of this page)
Here is what to read if none of your peripheral neuropathy symptoms fit in the normal box of numbness, tingling, burning, cold, strength, and balance. What if you have redness? Swelling? Blotchy skin? Hair loss?
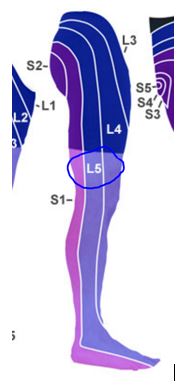
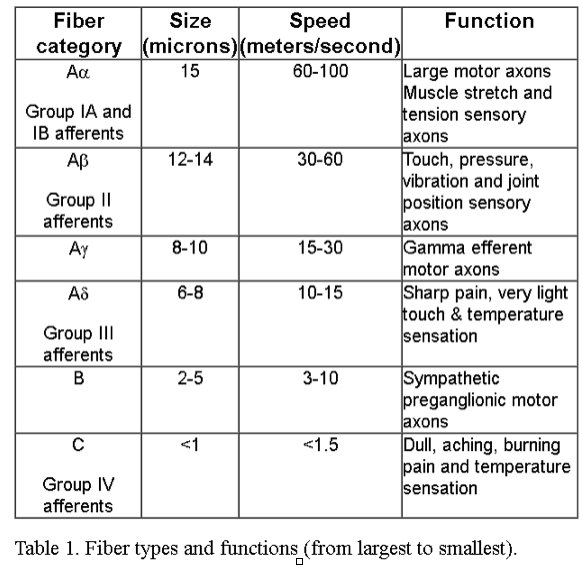
Peripheral neuropathy can damage sensory fibers which cause symptoms like pain, tingling, balance issues and numbness. It can damage motor peripheral fibers which result in weakness and balance issues. It can also damage your autonomic fibers. These are called your sympathetic and parasympathetic fibers and they control things like blood pressure, heart rate, sweating etc.
“Diabetic autonomic neuropathy (DAN) is a serious and common complication of diabetes but remains among the least recognized and understood”1
Keep in mind that diabetic neuropathy is likely the most studied systemic neuropathy but that in practice these same symptoms are common in other causes such as chemotherapy, autoimmune or even idiopathic (unknown) neuropathy.
“”¦and autonomic neuropathy (AN) is not unique to diabetes”¦”1
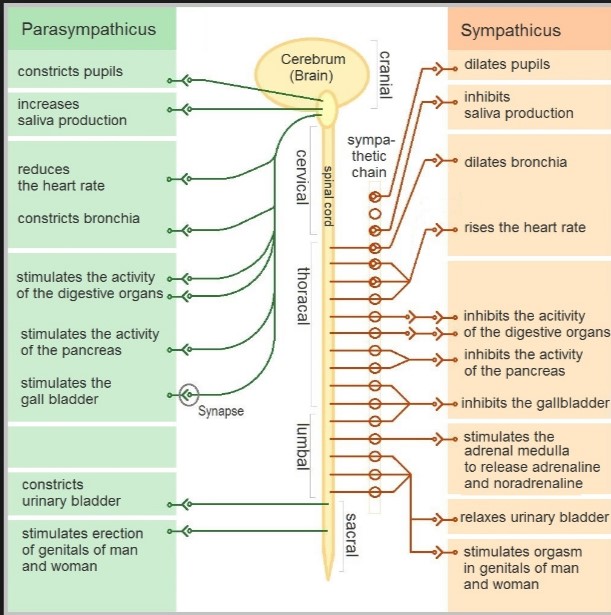
Here is a picture of what the two branches of your autonomic nervous system control. Image courtesy of:
https://en.wikipedia.org/wiki/Dysautonomia
Can this swelling or redness be caused by my neuropathy?Since I don’t want to write a graduate thesis on things, I will focus on two that we hear questions about the most.
In a nutshell, it can. Since the autonomic nerves control the microvasculature (capillaries), autonomic dysfunction can cause what is called “neuroedema” and “neuroischemia”. In other words, swelling and insufficient oxygen from a neurological cause instead of a vascular blockage. This does not mean that you can’t have swelling from a host of other causes like kidney or heart issues but that autonomic neuropathy can cause swelling as well.
I lost my hair on my legs / my toenails look funny
Autonomic neuroischemia affecting your capillaries ability to deliver oxygen and nutrients to the hair follicles can result in a loss of hair. Same thing for the nail beds.
The common presence of autonomic nerve involvement in peripheral neuropathy opens the door for the explanation of a host of symptoms outside just the sensory and motor fibers.
*Many quotations and information for this post come from this very excellent paper:
1NCBI Bookshelf. A service of the National Library of Medicine, National Institutes of Health.
De Groot LJ, Beck-Peccoz P, Chrousos G, et al., editors. Endotext [Internet]. South Dartmouth (MA):
MDText.com, Inc.; 2000-.
Diabetic Neuropathies
Aaron Vinik, MD, Carolina Casellini, M.D., and MarieLaure
Nevoret, M.D.
Timothy Kelm, DC, is one of the clinicians at Realief Medical PA. Since 2007 (or, as he would put it, before you ever saw an advertisement for neuropathy therapy) he has worked with many patients with peripheral neuropathy. He also trains new clinicians for Biolyst LLC, a medical company working for solutions to peripheral nerve damage. He has presented at the University of Minnesota Gynecological Oncology Research Symposium and participated in Tier One research with neuropathy therapy for laser treatment for neuropathy in regards to symptom control. He also lectures in the US to patients on peripheral neuropathy and neuropathy relief. He can be reached by contacting his patient coordinator via email, j.haley@realiefcenters.com or by phone 952-658-6354.